|
Identifying Sadists Among Female Sexual Offenders Using the Cumulative Scale of Severe Sexual Sadism
Dawn M. Pflugradt1, Bradley P. Allen2
1 Wisconsin Department of Corrections, USA
2 Sand Ridge Secure Treatment Center, USA
[Sexual Offender Treatment, Volume 8 (2013), Issue 1]
Abstract
Among the most common reasons cited for the scarcity of research on female sexual perpetrators has been the relatively small number of adjudicated female sex offenders, socio-cultural factors, and lack of gender specific diagnostic criteria. These issues are magnified when sub-categories of sex offenders are examined such as sexual sadism which is considered one of the rarest paraphilias. This paper examined: if the Cumulative Scale of Severe Sexual Sadism distinguished female sexual sadists from nonsadistic sex offenders and if sadistic behaviors were comparable for male and female sexual sadists. The coding of these items was done using archival data such as criminal complaints, police reports and sexual offender assessments. The criterion was a clinical diagnosis of sexual sadism which was present for 5 individuals. Using a cut-off of 4 points, the total score of the scale identified all female sexual sadists correctly whereas only two of the presumably nonsadistic female offenders were false positive cases. Upon closer inspection of their case files, however, these two cases could also be diagnosed with sexual sadism. The relative frequencies differed strongly from the corresponding values for males which may indicate gender-specific differences in the expression this disorder. The sadism scale thus appeared to be a viable aid for diagnosing sadism in female sexual offenders. Implications for further research were discussed.
Key Words: Assessment, female sexual offenders, sexual deviancy, sadism, sexual sadism
scale
Background
Although perceived as an elusive concept to define and measure, the essential diagnostic criteria of sexual sadism, since first being documented by Krafft-Ebing (1886), have basically remained unchanged (Knoll & Hazelwood, 2009; Yates, Hucker, & Kingston, 2008; Proulx, Blais & Beauregard, 2006). Specifically, the central enduring element of sexual sadism, the derivation of sexual pleasure from inflicting pain (both physical and psychological) onto another person, has been retained in the current major diagnostic taxonomies (DSM-IV-TR; American Psychiatric Association, 2000; ICD-10; World Health Organization, 2004). As described by Krafft-Ebing (1886) in his classic work, Psychopathia Sexualis:
The quality of sadistic acts is defined by the relative potency of the tainted individual. If potent, the impulse of the sadist is directed to coitus, coupled with preparatory, concomitant or consecutive maltreatment, even murder, of the consort ("Lust Murder"), the latter occurring chiefly because sensual lust has not been satisfied with consummated coitus. (p. 53)
Subsequent descriptions of male sadists expanded upon these early conceptualizations and two additional characteristics were determined to be essential features of sexual sadism: feelings of power and control and violent sexual fantasies (Yates et al., 2008; Proulx et al., 2006; MacCulloch, Snowden, Woods & Mills, 1983). For sadists, the infliction of pain is not an end in itself, but the means by which to experience power and control accentuated by sexual gratification (Proulx et al., 2006). In psychodynamic terms, this behavior (of forcing someone to unwillingly succumb to physical and psychological pain) represents a process of objectification that allows the sadist to perceive himself as possessing the person (Fromm, 1977). Since the desire to control, as a primary motive for sadistic acts, may be exhibited in many different behaviors, of varying degrees, sadism may manifest itself in a variety of ways (MacCulloch, Snowden, Woods & Mills, 1983, p. 20). More recent research has indicated that sadistic behaviors may be better characterized by the humiliation of a victim(s) through the use of power and control rather than violence (Richards & Jackson, 2011).
The second common trait of male sexual sadists, the presence of violent sexual fantasies, appear to have a role in both the "genesis" and maintenance of sadistic behaviors (Yates et al., 2008, MacCulloch, Snowden, Woods & Mills, 1983). Although "...at least some normal men indulge in sadistic fantasies" (MacCulloch et al., 1983, p. 27), Proulx, Blais and Beauregard (2006) proposed that the personality profile of sexual sadists results in feelings of inferiority, rejection and humiliation. When he experiences distress or becomes disinhibited, a sadist may "actualize" his fantasies by engaging in a sexually sadistic offense to resolve or alleviate internal stress. After engaging in the sadistic behaviors, the deviant behaviors are maintained by fantasy which become a cue for sexual response (MacCulloch et al., 1983). It is important to note, however, that while explanations of sadistic sexual fantasies based upon personality and learning theories may be applicable to the maintenance and escalation of deviant behaviors, they do not explain how these fantasies are initially developed (MacCulloch et al., 2000). As stated by MacCulloch and colleagues: "...it seems unlikely that there is any single universal causative factor" (MacCulloch et al., 1983, p.27).
Although sexual sadism, as a theoretical construct, has been relatively consistent over time, its operationalization or application as a diagnosis has been criticized for being limited by numerous factors including variable estimates of prevalence (Nitschke, Osterheider & Mokros, 2009), poor predictive validity pertaining to recidivism risk (Kingston, Seto, Firestone & Bradford, 2010) and diagnostic unreliability (Yates et al., 2008). Perhaps one major challenge relating to the accurate diagnosis of sexual sadism as a paraphilia is the presence of non-pathological sadomasochistic interests and behaviors for most participants (Richters, J., De Visser, R.O., Rissel, C.E., Grulich, A.E., & Smith, A.M.A., 2008). In a telephone interview of 19,307 respondents 16-59 years of age, Richters and colleagues found that 1.8% of sexually active people (2.2% men and 1.3% women of total sample) had been involved in sadomasochism during the previous year. As they further found for these respondents, sadomasochism was not associated with psychological distress, sexual difficulties or a pathological symptom of past abuse. In a similar study of a sample of 367 male volunteers, 40 to 79 years of age, Ahlers and colleagues found that 62.4% reported at least one paraphilia-associated sexual arousal pattern (Ahlers, Schaefer, Mundt, Roll, Englert, Willich & Beier, 2011). As they concluded, for males, paraphilia related behaviors cannot be regarded as unusual from a normative perspective.
Whereas there is a paucity of information regarding the prevalence sexual sadism for females (Logan, 2008), there has been some research which examined the prevalence and role of women in the sadomasochistic subculture (Breslow, Evans & Langley, 1985). In an early study, Breslow and colleagues empirically investigated the prevailing view that females did not participate in the sadomasochistic or if they did, the numbers were too small to be analyzed. Based upon the responses on questionnaires which included 130 males and 52 females, they found that women comprised meaningful presence in the sadomasochistic subculture. Overall, they found that non-prostitute women participated in sadomasochistic sex and exhibited some similarities with non-prostitute heterosexual males. Both groups were similar in age, tended to be better educated and either remained unmarried or had higher divorce rates. In addition to other similarities, both male and females showed approximately the same degree of sexual interest in a large number of specific sexual acts. A notable difference, however, was that males discovered their sadomasochistic interests earlier in life while females were introduced to it by a sexual partner. Additionally, females also tended to engage in sadomasochistic sex more often with a greater number of partners.
Moreover, the diagnosis of sexual sadism is further complicated by inconsistencies with the current major diagnostic frameworks (Kingston & Yates, 2008). For example, the International Classification of Diseases, 10th Revision (ICD-10; World Health Organization, 1992), utilizes a dimensional approach which conceptualizes sexual sadism as: (1) an entity which suggests that passive and active wishes, that is, domination as opposed to submission, are combined; (2) indicative that some elements of sadomasochistic stimulation may be part of normal sexual activity (Nitschke, Mokros, Osterheider & Marshall, in press); and (3) a disorder whereby sadomasochistic arousal or sexual gratification is different from cruelty or anger in a sexual context (Berner, Berger & Hill, 2003). In contrast, the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (DSM-IV-TR; American Psychiatric Association, 2000), uses categorical criteria focusing on whether or not the dominant characteristics of sexual sadism are either present or absent (Kingston & Yates, 2008).
Recognizing the importance of accurately identifying sexual sadism, both as a public policy issue and human rights concern, Marshall and colleagues (Marshall, Kennedy, Yates, & Serran, 2002a; Marshall, Kennedy, & Yates, 2002b), conducted a series of studies to evaluate its diagnostic reliability. Not only did they conclude that the criteria used by clinicians to diagnose sexual sadism were inconsistent with both the ICD-10 and DSM-IV, the application of the criteria included "idiosyncratic" elements (Marshall et al., 2002a; Marshall & Kennedy, 2003). In response to these diagnostic inadequacies, Marshall and Hucker (2006) subsequently used a modified grounded theory approach to develop the Sexual Sadism Scale which is essentially a 17-item list of behavioral indicators determined to be associated with sexual sadism (see Table 1). As they suggested, "the scale serves both the needs of a categorical classification system, such as DSM or ICD, while at the same time employing the benefits of a dimensional system that has been touted by some as a better approach to diagnosis..." (2006, pg. 1).
Table 1: Marshall and Hucker’s Sexual
Sadism Scale |
| Item |
Offender is sexually aroused by sadistic acts
Offender exercises power/control/domination over the victim
Offender humiliates or degrades the victim
Offender tortures the victim or engages in acts of cruelty on victim
Offender mutilates sexual parts of the victim’s body
Offender has a history of choking consensual partners during sex
Offender engages in gratuitous violence toward victim
Offender has a history of cruelty to other persons or animals
Offender gratuitously wounds victim
Offender attempts to, or succeeds in, strangling, choking, or otherwise
asphyxiating victim
Offender keeps trophies (e.g., hair, underwear, ID) of victim
Offender keeps records (other than trophies) of offense
Offender carefully pre-plans offense
Offender mutilates nonsexual parts of the victim’s body
Offender engages in bondage with consensual partners during sex
Victim is abducted or confined
Evidence of ritualism in offense |
In follow up research, Nitschke and colleagues (2009) evaluated the psychometric properties of the Sexual Sadism Scale, particularly whether the criteria set conformed to a scale and if it differentiated sexually sadistic offenders from non-sadists. That is, they explored empirically whether the list of criteria put forward by Marshall and Hucker (2006) or a subset thereof would represent a cumulative scale. For this purpose, the criteria was scored dichotomously as either present (1) or absent (0). Their methodology incorporated two significant changes to the original scale which included: (1) changing the first item of the scale from "offender is aroused by sadistic acts" to "offender is sexually aroused to the act" which was made in order to prevent a circularity of argument; otherwise, the item content would presuppose what the scale was about to measure; and (2) and requiring at least three of the five "core" items (i.e., the first five items listed on the scale) for a diagnosis of sadism. After applying the modified scale to the archival data of 100 forensic patients committed to a high security hospital for mandatory treatment, they found "almost perfect" inter-rater reliability with "substantial concordance on the single item level..." (Nitschke et al. 2009, p.268). The resultant scale was also highly reliable and represented a strong scale of the Guttman type with no misclassifications, that is, it correctly distinguished sadists from non-sadists.
In a follow up study, Mokros, Schilling, Eher and Nitschke (2012), replicated the structure of the original 11-item set indicative of severe sexual sadism with a sample of 105 sexual offenders from Austria, 18 of whom had a diagnosis of sexual sadism. Although the deterministic properties identified in the original sample couldn't be confirmed, the items corresponded to a one parameter logistic model. Thus, the set of items retained the properties of a cumulative scale with a total score as a sufficient statistic for an underlying trait (Mokros et al. 2012). The reliability estimates, specificity and sensitivity were lower than the original sample, however, but still within an acceptable standard for making clinical decisions. That is, there was good criterion validity with the DSM-IV-TR diagnosis with a large effect size for distinguishing sadists from non-sadists. With a cut-off score of 7, as compared to 4 for the original sample, the sensitivity and specificity estimates were 56% and 90% respectively.
In addition to validating Marshall and Hucker's (2006) criteria for identifying sexual sadists, Nitschke et al. (2009) also provided two interesting implications in their analysis. The first was that their findings supported the notion that sexual sadism may best be described as a dimensional not categorical disorder, that is, as a range of symptoms/behaviors rather than simply being either present or absent. A second diagnostic consideration that can be drawn from their conclusions was that sexual sadism is the manifestation of a "latent trait" which "offers a unified explanation for overt behavior" (Nitschke et al., p. 268).
Although significant advances have been made in developing empirically derived assessment practices for male sexual perpetrators, the identification of risk and treatment needs for female sexual offenders is extremely limited (Cortoni, 2010; Cortoni, Hanson & Coache, 2010). Despite the scarcity of research in these areas, the risk factors for female sexual recidivism could plausibly include some of the same factors identified for males (Cortoni, Hanson & Coache, 2010). Available research, however, indicates that the way in which these factors are manifested by female sexual offenders are different from those exhibited male sexual perpetrators. This study applied the Cumulative Scale of Severe Sexual Sadism to a sample of 90 female sex offenders, which included some sexual sadists, previously diagnosed for clinical and not research purposes, in order to examine if there were common factors between male and female sexual sadists based upon the behavior manifestations of their offenses as well as to determine whether or not the scale could distinguish those females previously diagnosed with Sadism from those without the diagnosis. The hypotheses for this study included: - The cumulative scores of the severe sexual sadism scale distinguished female sexual sadists from non-sadistic sexual offenders;
- The relative frequency of the individual items of the severe sexual sadism scale were comparable for male and female sexual sadists
Method
Participants
This study utilized archival data for 90 convicted female sexual offenders incarcerated in a mid-western medium/maximum security prison during 2010-2011. The information included: complaints; police and probation/parole agent reports; sentencing transcripts; and sexual offender assessment(s). The records also contained both self-reports from the offenders as well as witness and victim reports/descriptions of the sexual offenses. As noted, the offenders' self-reports were generally consistent with other information found in the file. Included in the sample of 90 female sexual offenders, five offenders had a diagnosis of sexual sadism which was determined prior to their inclusion in this research study. The diagnosis of sadism was given by psychologists, at admission to the prison, based upon a consensus that they fulfilled the DSM-IV TR criteria utilizing documented offense history of inflicting physical violence upon victims and self-reports of associated sexual arousal. Demographic information for the sample was derived from when the offender committed the index sexual offense. As indicated in the records, the average age of the subjects at the time of the index sexual offense was 30.6 years SD= 10.33; range=17-74 years) with 26 (29%) having graduated from high school, 46 ( 51%) with less than a high school education and 18 (20%) having a post-high education. Regarding marital status, 47 (52%) subjects were single, 35 (39%) divorced or separated and 8 (9%) were married. Lastly, 17 (19%) of the subjects were African American, two (2%) were Hispanic and 71 (79%) were Caucasian.
Demographic information for this sample is consistent with what is generally known about the demographics of female sexual offenders in general. Specifically, common demographics indicate that many tend to be white, single women between the ages of 26 and 36 years old, with low socioeconomic status (Sandler & Freeman, 2007; Sandler & Freeman, 2009; Turner, Miller, & Henderson, 2008).
Analysis
The data was analyzed by first examining if Nitschke et al.'s (2009) Cumulative Scale of Severe Sexual Sadism discriminated between female sex offenders diagnosed with sexual sadism and female offenders convicted of a sexual offense who were not identified as sexual sadists. The authors of this study scored the sadism scale on all 90 subjects. Since there were a relatively small number of female sexual sadists in the sample, the analysis qualitatively compared demographic characteristics of female sadists and non-sadists, the frequency distribution of total scores and the frequency distribution of individual items between males and females.
The data was further analyzed using nonparametric procedures which included calculating the area under the curve (AUC) from the receiver operating curve characteristic (ROC). The ROC curve is approximated by connecting the data points (sensitivity, 1-specificity) and then calculating the estimated area under the curve (AUC) using the trapezoidal rule (Lasko, Bhagwat, Zou & Ohno-Machada, 2005). By using this nonparametric method, the calculated AUC has been shown to be equivalent to the Mann-Whitney U statistic normalized by the number of possible pairings. It imposes no structural assumptions on the data and allows for the calculations of confidence intervals. Additionally, a Fisher exact test was used which is a nonparametric statistical significance test to measure the relative proportion of categorical data using a 2x2 contingency table. Specifically, this procedure was utilized to test the null hypothesis that the relative proportions of the individual items of the Cumulative Scale of Severe Sexual Sadism were independent for male and female sexual sadists.
Results
Demographic characteristics for the total sample are summarized below in Table 2.
Table 2: Sample Demographics (N=90) |
| Age |
Range = 17-74 years |
Mean = 30.6 |
SD = 10.33 |
| Ethnicity |
African American = 17 (19%) |
Hispanic = 2 (2%) |
Caucasian = 71 (79%) |
| Education |
Less than High School = 46 (51%) |
High School = 26 (29%) |
Post High School = 18 (20%) |
| Marital Status |
Married = 8 (9%) |
Single = 47 (52%) |
Divorced/Separated = 35 (39%) |
Of the five subjects diagnosed with sexual sadism, the mean age at which the women began their assaultive behaviors was 25.2 years (SD: 8.04; range 21-33 years). The educational level of the offenders ranged from some high school (n=4) to completion of high school (n=1). The women's executive functioning abilities were intact as indicated by scores within the average range on the Stroop and Trail-making tests (Pflugradt & Allen, 2010). Collectively, the women's victims included one female and four male children, an adolescent female, an adult female and an adult male. In addition to a diagnosis of sexual sadism, it is important to note that none of the subjects had other major mental health diagnoses. Although applicable mental health diagnoses for all of the subjects were considered for inclusion in this study, it determined that the reliability wasn't at a level that would provide any meaningful information. However, all of the subjects diagnosed with sexual sadism had co-offenders (relatively few of the non-sadists, that is n=15, had co-offenders). In addition, whereas all of the subjects with sexual sadism had relationships with their victims (often as caregivers, n=4), about a third (n=32) of the non-sadist subjects had similar type of relationships with the persons whom they assaulted.
The scoring of the scales, completed by the authors of this study, resulted in an inter-rater reliability of 94%. The disagreement between three of the items across three subjects was discussed and resolved prior to determining finals scores. The three items upon which the scorers initially disagreed were "Offender mutilates non-sexual parts of the victim's body" and "Offender mutilates sexual parts of the victim's body." In regard to the mutilation of non-sexual body parts, the issue revolved around whether the infliction of physical harm was mutilation and whether it was part of the sadistic behaviors. The discrepancy was resolved by examining the offenders' offense behaviors and patterns and determining how closely they matched the infliction of physical harm. Similar to the previous item, the disagreement regarding mutilating sexual body parts pertained to what constituted "mutilation" and "sexual" parts. Again, the scorers were able to reach consensus after considering the behavioral patterns of offender's sadistic offense.
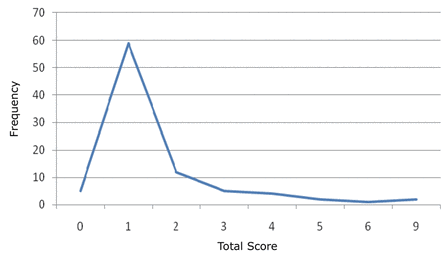
At a cut-of score of 4, inclusive of at least three items from the core group, Nitschke et al.'s scale accurately identified all of the female sexual sadists in the sample with a sensitivity of 1.00. At the same cutoff score, the specificity of the scale (.986) was not as accurate with two false positives, but still considered to be at an acceptable level. Without the additional coding rule of requiring at least three core criteria, however, the specificity of the scale decreases to 95.3%. As illustrated by Figure 1, the distribution of the total scores was skewed to the right with a majority of subjects (59) having a total score of one. The second most frequent score, however, dropped sharply with 12 subjects having a total score of two. Interestingly, without the requirement for at least three of the five core items, the scale would have identified only two additional subjects as sexual sadists.

| | Figure 1: Distribution of Total Scores |
The relative frequencies of Nitschke et al.'s (2009) original scale items were compared to those obtained for the female sexual offenders and summarized in Table 2. As illustrated, the relative frequency of the items between genders was relatively dissimilar with the exception of two low occurring items (i.e., "Insertion of object(s) into victim's bodily orifice(s)" and "Offender keeps trophies of the victim or keeps records of the offense"). In addition, the relative frequency of only one item was greater for female offenders, that is, "Offender is sexually aroused by the act" which was modified from the original "Offender is sexually aroused by sadistic acts."
Table 3: A Comparison of Relative
Frequency of Items by Gender |
| Item |
Male |
Female |
Fisher’s
Exact Test |
| Offender engages in gratuitous violence toward or wounding
of the victim |
.76 |
.11 |
p<.01 |
| Offender exercises power/control/domination over the
victim |
.57 |
.17 |
p<.01 |
| Offender humiliates or degrades the victim |
.53 |
.09 |
p<.01 |
| Offender is sexually aroused by the act (modified from
the original “Offender is sexually aroused by sadistic acts”) |
.50 |
.93 |
p<.01 |
| Offender tortures the victim or engages in acts of cruelty
to the victim |
.44 |
.04 |
p<.01 |
| Evidence of ritualism in offense |
.38 |
.01 |
p<.01 |
| Victim is abducted/ or confined |
.37 |
.09 |
p<.01 |
| Insertion of object(s) into victim’s bodily orifice(s) |
.12 |
.09 |
p=.32* |
| Offender mutilates sexual parts of the victim’s
body |
.08 |
.03 |
p=.14* |
| Offender mutilates nonsexual parts of the victim’s
body |
.08 |
.02 |
p<.01 |
Offender keeps trophies (e.g., hair, underwear, ID)
of the victim or keeps records of the offense
|
.03 |
.06 |
p=.19* |
| *not significant at p<.06 level |
The area under the curve calculation indicated that the Cumulative Scale of Severe Sexual Sadism discriminated the two groups, that is, subjects with a diagnosis of sexual sadism and those sexual offenders not identified as sadists. The area under the curve coefficient was .986 with a 95% confidence interval of .935-.999 which is significant at the p< .01 level. The results of the Fisher exact test indicated that the proportion of sadistic characteristics for males, on most of the items, were significantly greater than the female sexual offenders with three exceptions. As illustrated in Table 3, the proportion of males and females responses for the items "Insertion of object(s) into victim's bodily orifice(s)," "Offender mutilates sexual parts of the victim's body" and "Offender keeps trophies (e.g., hair, underwear, ID) of the victim or keeps records of the offense" were not significantly different.
Discussion
Nitschke et al.'s Cumulative Scale of Sexual Sadism accurately identified the five female sexual sadists, according to DSM-IV TR diagnostic criteria, included in an opportunity sample sample of 90 incarcerated female sex offenders. The female sexual sadists total scores included eight (two offenders with five core items), six (one offender with four core items) and four (two offenders with three core items). These results are consistent with Nitschke et al.'s application of the scale to male sexual sadists which also yielded perfect sensitivity. The scale also identified two additional female subjects who were not diagnosed with sexual sadism previously. As a result of the elevated scores for these two subjects, the authors further reviewed the records and found that they actually fulfilled the diagnostic criteria for sexual sadism. Whereas there may be several reasons why these subjects were not diagnosed with sadism at intake into the prison, the most likely explanation was that their deviant sexual arousal was not readily documented in the available police reports and was not disclosed during interview. It was only after a more in-depth file review which included additional information and self- disclosures documented by prison clinical staff that it became evident that these subjects had exhibited sadistic behavioral patterns, during the index offense, for at least a six month period. The authors followed up with the clinical staff of the sample participants. The follow-up indicated that no additional women (who were not identified by the scale) self-reported or where identified by staff as meeting criteria for sexual sadism. This finding further supports the conclusion that the severe sadism scale would be an effective diagnostic instrument to screen female sexual offenders for the presence of sexual sadism.
A qualitative examination of the relative frequencies yielded mixed results with the greatest discrepancies occurring between the "core" behaviors. Thus, even though the total score of the scale effectively discriminated sadistic from non-sadistic sex offenders, the behaviors between genders varied substantially. Whereas there may be many ways to interpret these results, this information is consistent with a hypothesis that sexual sadism does exist in females.
These findings are also supportive of a previous study by the authors which employed a qualitative application of the Sexual Sadism Scale to evaluate the behavioral characteristics of female sexual sadists. The authors of the previous study found that sadistic behaviors expressed by female sexual sadists included at least 11 of the 17 items. Despite these similarities with male sadists, however, the grounded theory analysis also identified several behavioral characteristics that appeared gender specific to female sadists (Pflugradt & Allen, 2012).
In particular, female sexual sadists usually committed their assaults with a co-offender and they had a relationship with the victim(s). Additional characteristics included: the offender appearing to experience vicarious sexual arousal to manipulating the victim(s) and co-offender; the offender was often in a caregiver role; offender exhibiting greater arousal to the psychological components of the sadistic acts; and the exertion of control by the offender included goal oriented nurturance to create emotional dependence in the victim(s). These preliminary findings suggested that as compared to male sadists, female sexual sadism was possibly a more complex, multi-factorial construct that encompasses a wide range of behaviors, cognitive processes and emotional responses (Pflugradt & Allen, 2012; Cortoni et al. 2010).
Although the results of this study are not easily generalizable, primarily due to a small sample size (although large for female sadists and female sexual offenders), it hopefully provides some further/additional insight onto the behavioral representations of female sexual sadism. Furthermore, the sample was also susceptible to selection bias, that is, included only incarcerated female sexual offenders, resulting in a much greater prevalence (7.8%) than would be expected in a more representative sample inclusive of offenders on community supervision. As mentioned, these findings, along with other preliminary research on female sex offenders, seem to point to unique behavioral expressions or patterns of psychological characteristics shared with male sex offenders, though often not to the same extent or degree. Rather, female sexual offenders also appear to possess unique qualities that have not yet been completely identified and/or are not fully understood such as deficits in the ability to form and maintain appropriate intimate relationships (i.e., victimizing individuals within a pseudo family structure). Moreover, female sexual offending seems to involve a contextual dimension such that the offending behaviors are often in relationship with others who share a socio-emotional bond or connection.
As the research on female sexual offenders continues to grow with increased interest and improved research methodologies, it will likely be possible to further elaborate upon these other dimensions in the near future. Perhaps, even more importantly, further research will provide opportunities to explore the relationships between them and how they interact. Until then, however, the examination of the underlying dynamics of female sexual offending will likely continue to be based upon comparisons with male sexual perpetrators that are hopefully generated by empirical investigation.
Author Note
Portions of this article were presented during a poster session at the 30th Annual Conference of the Association for the Treatment of Sexual Abusers (ATSA), Toronto, Canada (November 2011).
References- Acton, G.S., & Zodda, J.J. (2005). Classification of psychopathology: Goals and methods in an empirical approach. Theory and Psychology, 15, 373-399.
- Ahlers, C.J., Schaefer, G.A., Mundt, I.A., Roll, S., Englert, H., Willich, S.N., & Beier, K.M. (2011). How unusual are the contents of paraphilias? Paraphilia-associated sexual arousal patterns in community-based sample of men. Journal of SExua Medicine, 8, 1362-1370. Doi:10.1111/j.1743-6109.2009.01597.x.
- American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders, fourth edition, text revision. Washington, DC: Author.
- Berner, W., Berger, P., & Hill, A. (2003). Sexual sadism. International Journal of Offender Therapy and Comparative Criminology, 47, 383-395.
- Breslow, N., Evans, L., & Langley, J. (1985). On the prevalence and roles of females in the sadomasochistic subculture: Report of an empirical study. Archives of Sexual Behavior, 14, 303-317.
- Cortoni, F., Hanson, R.K., & Coache, M-E. (2010). The recidivism rates of female sexual offenders are low: A meta-analysis. Sexual Abuse: A Journal of Research and Treatment, 22, 387-401.
- Cortoni, F. (2010). The assessment of female sexual offenders. In T.A. Gannon & F. Cortoni (Eds.), Female sexual offenders: Theory, assessment, and treatment. John Wiley & Sons. (pp. 87-100).
- Fromm, E. (1977). The anatomy of human destructiveness. New York: Holt.
- Kingston, D.A., Seto, M.C., Firestone, P., & Bradford, J.M. (2010). Comparing indicators of sexual sadism as predictors of recidivism among adult male sexual offenders. Journal of Consulting and Clinical Psychology, 4, 574-584.
- Kingston, D.A. & Yates, P.M. (2008). Sexual sadism: Assessment and treatment. In Richard Laws & W.T. O'Donohue (Eds.), Sexual deviance: Theory, assessment, and treatment, second edition (pp. 231-243). New York: Guilford Press.
- Knoll, J.L. & Hazelwood, R.R. (2009). Becoming a victim: Beyond sadism in serial murders. Aggression and Violent Behavior, 14, 106-114.
- Krafft-Ebing, R. (1886). Psychopathia Sexualis. (F.J. Rebman translation, 1906) New York: Rebman Co.
- Lasko, T.A., Bhagwat, J.G., Zou, K.H., & Ohno-Machado, L. (2005). The use of receiver operating characteristic curves in biomedical informatics. Journal of Biomedical Informatics, 38, 405-415.
- Logan, C. (2008). Sexual deviance in females: Psychopathology and theory. In Richard Laws & W.T. O'Donohue (Eds.), Sexual deviance: Theory, assessment, and treatment, second edition (pp. 486-507). New York: Guilford Press.
- MacCulloch, M., Gray, N. & Watt, A. (2000). Britian's sadist murderer syndrome reconsidered: An associative account of aetiology of sadistic sexual fantasy. Journal of Forensic Psychiatry, 11, 401-418.
- MacCulloch, M.J., Snowden, P.R., Woods, P.J.W., & Mills, H.E. (1983) Sadistic fantasy, sadistic behavior and offending. British Journal of Psychiatry, 143, 20-29.
- Marshall, W.L., Fernandez, Y.M., Marshall, L.E. & Serran, G.A. (2006). Sexual offender treatment: Controversial issues. Chichester, West Sussex, England: John Wiley and Sons.
- Marshall, W.L., & Hucker, S.J. (2006). Issues in the diagnosis of sexual sadism. Sexual Offender Treatment, 1 (2). Available online: http://www.sexual-offender-treatment.org.
- Marshall, W.L., & Kennedy, P. (2003). Sexual Sadism: An elusive diagnosis. Aggression and Violent Behavior, 8, 1-22.
- Marshall, W.L., Kennedy, P., Yates, P., & Serran, G. (2002a). Diagnosing sexual sadism in sexual offenders: Reliability across diagnosticians. International Journal of Offender Therapy and Comparative Criminology, 46(6), 668-677.
- Marshall, W.L., Kennedy, P., & Yates, P. (2002b). Issues concerning the reliability and Validity of the diagnosis of sexual sadism applied in prison settings. Sexual Abuse: A Journal of Research & Treatment, 14(4), 301-311.
- Miller, H.A., Turner, K., & Henderson, C.E. (2009). Psychopathology of sex offenders: A comparison of males and females using latent profile analysis. Criminal Justice and Behavior, 36, 778-792.
- Mokros, A., Schilling, F., Eher, R. & Nitschke, J. (2012). The severe sexual sadism scale: Cross- validation and scale properties. Psychological Assessment, 24, 764-769.
- Nitschke, J., Mokros, A. Osterheider, M. & Marshall, W.L. (in press). Sexual sadism: Current diagnostic vagueness and the benefit of behavioral definitions. International Journal of Offender Therapy and Comparative Criminology. DOI: 10.1177/0306624X12465923.
- Nitschke, J., Osterheider, M. & Mokros, A. (2009). A cumulative scale of severe sexual sadism. Sexual Abuse: A Journal of Research & Treatment, 21(3), 262- 278.
- Pflugradt, D.M. & Allen, B.P. (2010). An exploratory analysis of executive functioning for female sexual offenders: A comparison of characteristics across offense typologies. Journal of Child Sexual Abuse, 19, 434-449.
- Pflugradt, D.M. & Allen, B.P. (2012). A grounded theory analysis of sexual sadism in females. Journal of Sexual Aggression, 18, 325-337.
- Proulx, J., Blais, E., & Beauregard, E. (2006). Sadistic sexual aggressors. In W.L. Marshall, Y.M. Fernanadez, L.E. Marshall & G.A. Serran (Eds.) Sexual Offender Treatment: Controversial Issues (pp. 61-77). West Sussex England: John Wiley and Sons.
- Richards, H. & Jackson, R.L. (2011). Behavioral discriminators of sexual sadism and paraphilia nonconsent in a sample of civilly committed sexual offenders. International Journal of Offender Therapy and Comparative Criminology, 55, 207-227.
- Richters, J., De Visser, R.O., Rissel, C.E., Grulich, A.E., & Smith, A.M.A. (2008). Demographic and psychosocial features of participants in bondage and discipline, "sadomasochism" of or dominance and submission (BDSM): Data from a national survey. Journal of Sexual Medicine, 5, 1660-1668. doi: 10.1111/j.1743-6109.2008.00795.x
- Sandler, J.C. & Freeman, N.J. (2007) Typology of female sex offenders: A tests of Vandiver and Kercher. Sex Abuse, 19, 73-89.
- Sandler, J.C. & Freeman, N.J. (2009). Female sex offender recidivism: A large-scale empirical Analysis. Sexual Abuse: A Journal of Research and Treatment, 21, 455-473.
- Turner, K., Miller, H., & Henderson, C. (2008). Latent profile analysis of offense and personality Characteristics in a sample of incarcerated female sexual offenders. Criminal Justice and Behavior, 35, 879-894.
- World Health Organization (1992). The ICD-10 classification of mental and behavioral Disorders: Clinical descriptions and diagnostic guidelines. Geneva, Switzerland: Author.
- Yates, P. M., Hucker, S. J., & Kingston, D. A. (2008). Sexual sadism: Psychopathology and theory. In D. R. Laws, & W. T. O'Donohue (Eds.), Sexual deviance: Theory, assessment, and treatment (2nd ed.) (pp.213-230). New York: Guilford.
Author address
Dawn M. Pflugradt
Psychological Services Unit
Taycheedah Correctional Institution
PO Box 1947
Fond du Lac
WI 54936
dawn.pflugradt@wisconsin.gov
|